Angina pectoris - en oversikt
Angina pectoris er brystsmerter som oppstår under og etter fysiske anstrengelser og/eller emosjonelt stress, oftest med kortere varighet enn 15 minutter og som skyldes redusert blodforsyning til hjertemuskelen.

Sist oppdatert:
12. okt. 2021
Innhold i artikkelen
Hjertet

Hjertet er en kraftig muskel. Det indre av hjertet er delt opp i fire kammer, to forkammer og to hjertekammer. Oksygenfattig blod kommer inn i høyre forkammer og pumpes ut i lungekretsløpet fra høyre hjertekammer. Oksygenrikt blod kommer inn i venstre forkammer og pumpes ut i det store kretsløpet fra venstre hjertekammer. Hjertets muskelsammentrekninger styres og samordnes av elektriske signaler som passerer gjennom et elektrisk ledningsnett som ligger inne i hjertemuskulaturen.
Når vi anstrenger oss, må hjertet pumpe kraftigere og raskere for å bringe nok blod rundt til muskulaturen og de andre organene i kroppen. For å klare det, trenger hjertet mer næring og oksygen, derfor må også blodforsyningen til hjertemuskelen øke. Et friskt hjerte kan øke blodstrømmen til kransårene (koronararteriene) til det ni-dobbelte av hva den er i hvile. Siden hjertet er en stor muskel som arbeider hele tiden, behøves kontinuerlig tilførsel av oksygen og næring. Denne tilførselen skjer via blodet. Fra første del av hovedpulsåren avgår to kransårer (høyre og venstre koronararterie) som forløper på utsiden av hjertemuskulaturen. Koronararteriene deler seg etter hvert opp i stadig mindre grener som "dukker ned" i muskulaturen og sørger for blodforsyningen til alle deler av hjertet.
Hva er angina pectoris?

Angina pectoris er anfall med brystsmerter som skyldes redusert blodforsyning til hjertemuskelen. Anfallene utløses av fysiske anstrengelser eller sterke følelsesmessige reaksjoner, avtar raskt og forsvinner etter noen minutters hvile. Inntak av Nitroglycerin som smelter i munnen, gir smertelindring i løpet av 1-3 minutter.

Smerten ved angina beskrives som klemmende og sammensnørende, eventuelt som et trykk eller en varmefølelse over brystet. Den kjennes bak brystbeinet og kan stråle ut i venstre skulder og arm, noen ganger opp i kjeven. Anfallene utløses lettere når det er kaldt og etter et stort måltid.
Det er omtrent 100.000-150.000 angina-pasienter i Norge. Antall nye tilfeller per år er ca. 6 per 10.000.
Angina, årsak
 Økende aterosklerose
Økende ateroskleroseHjertemuskelen er som alt vev i kroppen, avhengig av stadig tilførsel av oksygen fra blodet. Smertene ved angina pectoris skyldes at hjertemuskelen får mindre oksygen enn den trenger, og oksygenmangel i muskulatur gir smerter.
Årsaken til at hjertet får mindre oksygen, er åreforkalkning (aterosklerose) som vil si at det er trange parti i blodårene som forsyner hjertet, de såkalte kransårene. Når hjertet jobber hardere, krever det mer oksygen, og på grunn av det trange partiet kommer det ikke tilstrekkelig blod til den aktuelle delen av hjertemuskelen. Dette er grunnen til at plagene forverres ved anstrengelser.
Flere faktorer gjør deg mer utsatt for å få angina pectoris:
- Høyt blodtrykk
- Høyt kolesterol
- Røyking
- Diabetes type 1 og type 2
- Lite mosjon
- Tendens til å reagere med aggresjon på stress
- Arvelige faktorer
- Høy alder
Menn får gjerne angina pectoris i yngre alder enn kvinner.
Angina, diagnostikk
Diagnosen kan ofte stilles med høy sannsynlighet ut fra de typiske symptomene. Dersom diagnosen er usikker, vil man foreta et belastnings-EKG. Dette er en test som gjøres under sykling på ergometersykkel, og slik test vil i mange tilfeller bekrefte diagnosen. Det kan også gjøres scintigrafisk undersøkelse av hjertet dersom EKG-undersøkelsen ikke gir tilstrekkelig avklaring.
Røntgenkontrast-undersøkelse av blodårene (hjertekateterisering) viser nøyaktig hvilke blodårer som er tette, og grad av tetthet. Dersom forholdene ligger til rette for det, kan hjertespesialisten i forbindelse med hjertekateteriseringen blokke ut det trange partiet av koronararterien. Som regel blir det også satt inn en stent som forhindrer at den trange åren lukker seg igjen.
Noen ganger lar det seg ikke gjøre å blokke ut den eller de trange koronararteriene. Da må det utføres bypass-operasjon.
Angina, behandling
 Hjerte - med infarkt
Hjerte - med infarktHensikten med behandlingen er å lindre smertene og forebygge hjerteinfarkt. Ved et hjerteinfarkt tilstoppes blodåren helt. Den delen av hjertemuskelen som dermed mister blodforsyningen, dør og erstattes med bindevev som mangler evnen til å arbeide som en pumpemuskel - hjertet blir med andre ord varig svekket i større eller mindre grad.
Egenbehandling
Det er flere ting du selv kan sørge for:
- Reduser inntaket av sukker og fett
- Prøv å opprettholde eller å øke din fysisk aktivitet, men unngå store fysiske anstrengelser, spesielt i kaldt vær
- Hvis du slutter å røyke, er det like gunstig som å bruke forebyggende medisiner
Medikamentell behandling
Det er et stort utvalg av legemidler som kan anvendes ved angina pectoris:
- Nitroglyserin som smeltes under tungen, lindrer eller fjerner smertene i løpet av få minutter ved at blodårene utvides. Medisinen er ufarlig selv om du kan få plagsom hodepine etter tablettinntak de første gangene. Du bør ta nitroglyserin til anfallet er helt over, selv om det medfører behov for å ta flere tabletter uten pause. Nitroglyserin finnes også i en langsomtvirkende tablettform for å forebygge anfall.
- Betablokkere minsker hjertemuskulaturens behov for oksygen, og beskytter mot altfor rask puls. Betablokkere virker forebyggende mot angina. Som alternativ til betablokker kan man bruke en type medisiner som kalles kalsiumblokkere.
- Acetylsalisylsyre anbefales til alle med angina. Det reduserer risikoen for å utvikle hjerteinfarkt ved å forebygge dannelse av blodpropp.
- Kolesterolsenkende medisiner (statiner) anbefales også til alle med angina. De reduserer risikoen for å utvikle hjerteinfarkt ved å bremse utviklingen av åreforkalkning (aterosklerose) og dermed forebygge dannelse av blodpropper.
Kirurgi

Dersom man ikke kommer til målet med medisiner og forebyggende tiltak, er det aktuelt med operasjon. Ved "bypass-operasjon" bruker man en blodåre fra leggen, eller en overflødig pulsåre i brysthulen, til å lage en ny vei forbi det trange stedet.
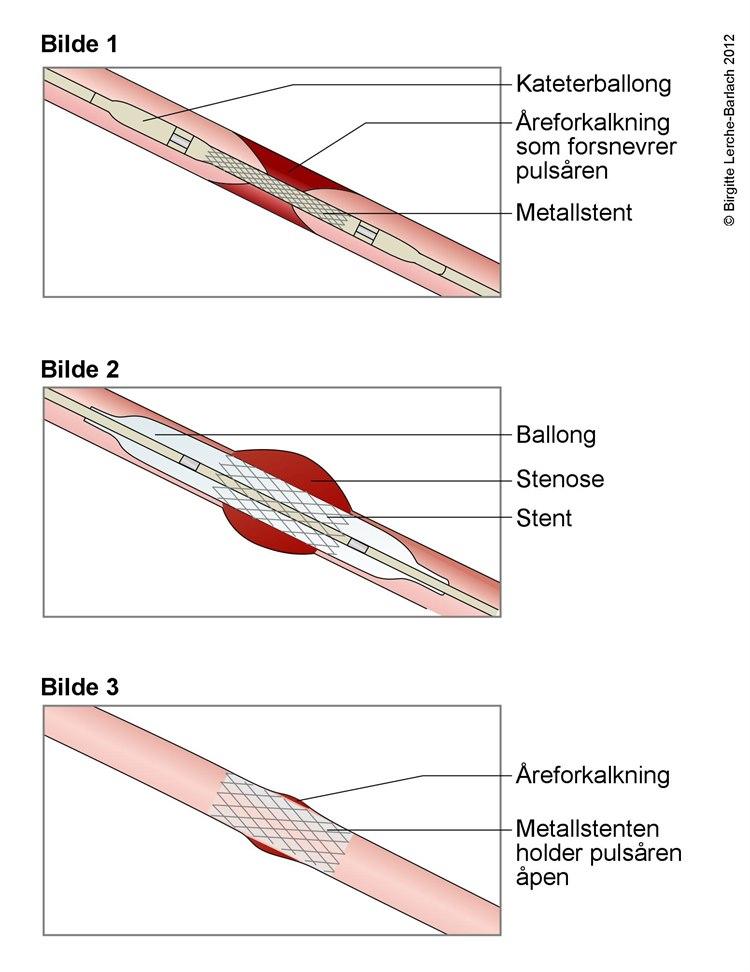 Stentbehandling av trang blodåre
Stentbehandling av trang blodåreVed PCI-teknikken stikker man en tynn slange (kateter) inn i en arterie ved håndleddet, eventuelt i lysken. Dette kateteret føres opp til hjertets blodårer (koronararteriene). En ballong i enden av slangen blåses opp når den er inne i det trange partiet. På denne måten kan man blokke ut trange blodkar. Det er også vanlig å sette inn en "armering" ("stent") i blodåren for å holde den åpen.
By-pass-operasjon er et stort inngrep som krever narkose og åpning av brystkassen. PCI gjøres med lokalbedøvelse på innstikkstedet og med våken pasient. I realiteten er det hjertespesialistene som avgjør og gir individuelle råd om hvilken behandlingsform som er anbefalt i det enkelte tilfellet.
Angina, prognose
Behandlingen sikter mot å bremse utviklingen av åreforkalkning og holde sykdommen stabil. Dersom man klarer å stabilisere tilstanden med røykeslutt, mosjon og medisiner, er prognosen god både på kort og lang sikt. Komplikasjonene man forsøker å forebygge er hjerteinfarkt og eventuelt hjertesvikt.
Angina kan føre til sykmelding og arbeidsuførhet, avhengig av hvor uttalt åreforkalkninger er, og i hvilken grad du er plaget. De aller fleste blir imidlertid med dagens moderne behandling symptomfrie - en bedring som kan vedvare lenge hvis det er rom for å tilpasse livsstilen.
Vil du vite mer
- Angina pectoris, årsaker
- Angina pectoris, symptomer
- Angina pectoris, når bør du søke hjelp
- Angina pectoris, inndeling
- Angina pectoris, undersøkelser og prøver
- Angina pectoris, behandling
- Angina pectoris, oppfølging og kontroller
- Ustabil angina pectoris
- Sekundærforebygging av koronarsykdom
- Landsforeningen for hjerte- og lungesyke
- Angina pectoris, brosjyre fra LHL på flere språk
- Arteriosklerose
- Høyt blodtrykk
- Høyt kolesterol
- Røyking
- Diabetes type 1
- Diabetes type 2
- Scintigrafisk undersøkelse
- Hjerteinfarkt
- PCI-teknikken
- Betablokkere
- Acetylsalisylsyre
- Statiner
Animasjoner
Dette dokumentet er basert på det profesjonelle dokumentet Kronisk koronare syndromer . Referanselisten for dette dokumentet vises nedenfor
- Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes: Developed by the task force for the management of chronic coronary syndromes of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2024. doi:10.1093/eurheartj/ehae177 DOI
- Ricci F, Banihashemi B, Pirouzifard M. et al. Familial risk of vasospastic angina: a nationwide family study in Sweden. Open Heart 2023; 10: e002504. pmid:38056914 PubMed
- Schef KW, Tornvall P, Alfredsson J, et al. Prevalence of angina pectoris and association with coronary atherosclerosis in a general population. Heart 2023. pmid:37225242 PubMed
- Folkehelseinstituttet. Hjerte- og karregisteret. Diagnoser 2018. statistikkbank.fhi.no
- Schoenhagen P, Ziada RM, Kapadia SP, Crowe TD, Nissen SE, Tuzcu EM. Extent and direction of arterial remodeling in stable versus unstable coronary syndromes: an intravascular ultrasound study. Circulation 2000; 101: 598-603. Circulation
- Halcox JP, Schenke WH, Zalos G, et al. Prognostic value of coronary vascular endothelial dysfunction. Circulation 2002; 106: 653-8. Circulation
- Sinha A, Dutta U, Demir OM, et al. Rethinking False Positive Exercise Electrocardiographic Stress Tests by Assessing Coronary Microvascular Function. J AM Coll Cardiol 2024; 83: 291-299. pmid:38199706 PubMed
- Opie LH, Commerford PJ, Bersh BJ. Controversies in stable coronary artery disease. Lancet 2006; 367: 69-78. PubMed
- Kaski JC. Pathophysiology and management of patients with chest pain and normal coronary arteriograms (cardiac syndrome X). Circulation 2004; 109: 568-72. Circulation
- Gotto AM jr., LaRosa JC, Hunninghake D, Grundy SM, Wilson PW, Clarkson TB et al. The cholesterol facts. A summary of the evidence relating dietary fats, serum cholesterol, and coronary heart disease. A joint statement by the American Heart Association and the National Heart, Lung and Blood Institute. Circulation 1990; 81: 1721-33. Circulation
- Lakka H-M, Lakka TA, Tuomilehto J, Salonen JT. Abdominal obesity is associated with increased risk of acute coronar events in men. Eur Heart J 2002; 23: 706-13. PubMed
- Rosengren A, Hawken S, Ôunpuu S, et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11 119 cases and 13 648 controls from 52 countries (the INTERHEART study): case-control study. Lancet 2004; 364: 953-62. PubMed
- Bogers RP, Bemelmans WJ, Hoogenveen RT, et al. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: A meta-analysis of 21 cohort studies including more than 300 000 persons. Arch Intern Med 2007; 167: 1720-8. PubMed
- Yusuf S, Hawken S, Ôunpuu S et al. Obesity and the risk of myocardial infarction in 27 000 participants from 52 countries: a case-control study. Lancet 2005; 366: 1640-9. PubMed
- Smith JK, Dykes R, Douglas JE, Krishnaswamy G, Berk S. Long-term Exercise and Atherogenic Activity og Blood Mononuclear Cells inPersons at Risk of Developing Ischemic Heart Disease. JAMA 1999; 281:1722-1727. Journal of the American Medical Association
- van der Meer RE, Maas AH. The Role of Mental Stress in Ischaemia with No Obstructive Coronary Artery Disease and Coronary Vasomotor Disorders. Eur Cardiol 2021; 16: e37. pmid:34721671 PubMed
- Tirosh A, Shai I, Tekes-Manova D et al. Normal fasting plasma glucose levels and type 2 diabetes in young men. N Engl J Med 2005; 353: 1454-62. New England Journal of Medicine
- Sattar N, Gaw A, Scherbakova O, et al. Metabolic syndrome with and without C-reactive protein as a predictor of coronary heart disease and diabetes in the West of Scotland Coronary Prevention Study. Circulation 2003; 108: 414-9. Circulation
- Prior JO, Quinones MJ, Hernandez-Pampaloni M, et al. Coronary circulatory dysfunction in insulin resistance, impaired glucose tolerance, and type 2 diabetes mellitus. Circulation 2005; 111: 2291-8. Circulation
- Fan C, Wang H, Gu Y. Recurrent Angina After Alcohol Consumption. JAMA Intern Med 2023. doi:10.1001/jamainternmed.2022.5411 DOI
- Bello N, Mosca L. Epidemiology of coronary heart disease in women. Prog Cardiovasc Dis 2004; 46: 287-95. PubMed
- Bugiardini R, Bairey Merz CN. Angina with "normal" coronary arteries: a changing philosophy. JAMA 2005; 293: 477-84. Journal of the American Medical Association
- Abrams J. Chronic stable angina. N Engl J Med 2005; 352: 2524-33. PubMed
- Sekhri N, Feder GS, Junghans C, et al. Incremental prognostic value of the exercise electrocardiogram in the initial assessment of patients with suspected angina: cohort study. BMJ 2008; 337: a2240. BMJ (DOI)
- The DISCHARGE Trial Group. CT or Invasive Coronary Angiography in Stable Chest Pain. N Engl J Med 2022. pmid:35240010 PubMed
- Papachristidis A, Vaughan GF, Denny SJ, et al. Comparison of NICE and ESC proposed strategies on new onset chest pain and the contemporary clinical utility of pretest probability risk score. Open Heart. 2020 May;7(1):e001081. doi: 10.1136/openhrt-2019-001081. PMID: 32467136. PubMed
- Maron DJ, Hochman JS, Reynolds HR, et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N Engl J Med 2020; 382: 1395-407. pmid:32227755 PubMed
- Benenati S, De Maria GL, Kotronias R, et al. Why percutaneous revascularisation might not reduce the risk of myocardial infarction and mortality in patients with stable CAD? Review. Open Heart 2023. doi:10.1136/openhrt-2023-002343 DOI
- von Koch S, Koul S, Grimfjärd P, et al. Percutaneous coronary intervention plus medical therapy versus medical therapy alone in chronic coronary syndrome: a propensity score-matched analysis from the Swedish Coronary Angiography and Angioplasty Registry. Heart 2024. pmid:39214681 PubMed
- Anderson L, Brown JP, Clark AM, Dalal H, Rossau HKK, Bridges C, et al. Patient education in the management of coronary heart disease. Cochrane Database Syst Rev 2017;6:CD008895. PMID: 28658719 PubMed
- Stead LF, Buitrago D, Preciado N, Sanchez G, Hartmann-Boyce J, Lancaster T. Physician advice for smoking cessation. Cochrane Database of Systematic Reviews 2013, Issue 5. Art. No.: CD000165. DOI: 10.1002/14651858.CD000165.pub4. DOI
- Barnoya J and Glantz SA. Cardiovascular effects of secondhand smoke: nearly as large as smoking. Circulation 2005; 111: 2684-98. Circulation
- Weitzman M, Cook S, Auinger P, et al. Tobacco smoke exposure is associated with the metabolic syndrome in adolescents. Circulation 2005; 112: 862-9. Circulation
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 2017. pmid:28304224 PubMed
- Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the management of patients with chronic coronary disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2023; 148: e9. PMID: 37471501 PubMed
- Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004; 364: 685-96. PubMed
- LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005; 352: 1425-35. New England Journal of Medicine
- Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in Patients with Chronic Coronary Disease. N Engl J Med. 2020 Aug 31. PMID: 32865380 PubMed
- Salazar CA, Basilio Flores JE, Veramendi Espinoza LE, et al. Ranolazine for stable angina pectoris. Cochrane Database Syst Rev. 2017 Feb 8;2:CD011747. doi: 10.1002/14651858.CD011747.pub2. (Review) PMID: 28178363 PubMed
- Al-Lamee RA, Nowbar AN, Francis DP. Percutaneous coronary intervention for stable coronary artery disease. Heart 2019; 105: 11-19. doi:10.1136/heartjnl-2017-312755 DOI
- Clar C, Oseni Z, Flowers N, Keshtkar‐Jahromi M, Rees K. Influenza vaccines for preventing cardiovascular disease. Cochrane Database of Systematic Reviews 2015, Issue 5. Art. No.: CD005050. DOI: 10.1002/14651858.CD005050.pub3. Accessed 01 February 2022. The Cochrane Library
- Udell JA, Zawi R, Bhatt DL, et al. Association between influenza vaccination and cardiovascular outcomes in high-risk patients: a meta-analysis. JAMA 2013 Oct 23;310(16):1711-20. PubMed
- Dibben G, Faulkner J, Oldridge N, Rees K, Thompson DR, Zwisler A-D, Taylor RS. Exercise‐based cardiac rehabilitation for coronary heart disease. Cochrane Database of Systematic Reviews 2021, Issue 11. Art. No.: CD001800. DOI: 10.1002/14651858.CD001800.pub4. Accessed 01 February 2022. The Cochrane Library
- Lagerros YT, Grotta A, Freyland S, et al. Risk of Death in Patients With Coronary Artery Disease Taking Nitrates and Phosphodiesterase-5 Inhibitors. J AM Coll Cardiol 2024; 83: 417-426. pmid:38233015 PubMed
- Hemingway H, Marmot M. Psychosocial factors in the primary and secondary prevention of coronary heart disease: a systematic review. I: Yusuf S, Cairns JA, Camm AJ, Fallen EL, Gersh BJ, red. Evidence based cardiology. London: BMJ Books, 1998: 269-85.